Zoonosis, or the jump from an animal virus to humans, has the characteristics of a contingent event. In principle, this leap can be limited by sanitary control of domestic animal species and by regulation of trade, contact and consumption of wild species. However, given the complexity of modern society and the close contact between humans at a global level, the probability of a virus jump to humans is not an avoidable event, so zoonosis can be considered a contingent phenomenon.
This situation has been clearly shown in recent times with the appearance of MERS (MERS-Cov), SARS (SARS-Cov) and recently the COVID-19 (SARS-Cov-2). This propagation is fundamentally motivated by globalization, although the factors are multiple and complex, such as health controls and the structure of livestock farms. But the list is long, and we can also mention the expansion of other viral diseases due to climate change, such as Zika, Chikungunya or Dengue.
The question that arises in this scenario is: What factors influence the magnitude and speed of the spread of a pandemic? Thus, in the cases mentioned above, a very significant difference in the behavior and spread of infection can be seen. Except in the case of COVID-19, the spread has been limited and outbreaks have been localized and isolated, avoiding a global spread.
In contrast, the situation has been completely different with CoVID-19. Thus, its rapid expansion has caught societies unfamiliar with this type of problem unawares, so that health systems have been overwhelmed and without appropriate protocols for the treatment of the infection. On the other hand, authorities unaware of the magnitude of the problem, and ignorant of the minimum precautions to prevent the spread of the virus, seem to have made a series of chained errors, typical of catastrophic processes, such as economic bankruptcies and air accidents.
The long-term impact is still very difficult to assess, as it has triggered a vicious circle of events affecting fundamental activities of modern society.
In particular, the impact on health services will leave a deep imprint, with extension to areas that in principle are not directly related to the COVID-19, such as the psychological and psychiatric effects derived from the perception of danger and social confinement. But even more important is the detraction of resources in other health activities, having reduced the flow of daily health activity, so it is foreseeable a future increase in morbidity and mortality rates of other diseases, especially cancer.
To all this must be added the deterioration of economic activity, with reductions in GDP of up to two figures, which will trigger an increase in poverty, especially in the most disadvantaged segments of the population. And since the economic factor is the transmission belt of human activity, it is easy to imagine a perfect storm scenario.
Pandemic Influencing Factors COVID-19
But let’s return to the question that has been raised, about the singularity of SARS-Cov-2, so that its expansion has been unstoppable and that we are now facing a second wave.
To unravel this question we can analyze what the mathematical models of expansion of an infection show us, starting with the classic SIR model. This type of model allows us to determine the rates of infection (β) and recovery (γ), as well as the basic reproduction rate (R0=β/γ) from the observed morbidity.
The origin of the SIR models (Susceptible, Infectious, and Recovered) goes back to the beginning of the 20th century, proposed by Kermack and McKendrick in 1927. The advantage of these models is that they are based on a system of differential equations, which can be solved analytically and therefore suitable for resolution at the time they were proposed.
However, these types of models are basic and do not facilitate considerations of geographical distribution, mobility, probability of infection, clinical status, temporal development of each of the phases of the infection, age, sex, social distance, protection, tracking and testing strategies. On the other hand, the classic SIR model has a deductive structure, exclusively. This means that from the morbidity data it is possible to determine the basic reproduction rate exclusively, hiding fundamental parameters in the pandemic process, as will be justified below.
To contrast this idea, it is necessary to propose new approaches to the simulation of the pandemic process, as is the case of the study proposed in “A model of the spread of Covid-19” and in its implementation. In this case, the model is a discrete SIR structure, in which individuals go through an infection and recovery process with realistic states, in addition to including all the parameters for defining the scenario mentioned above, that is, probability of infection, geographical distribution of the population, mobility, etc. This allows an accurate simulation of the pandemic and, despite its complexity, its structure is very suitable for implementation with existing computational means.
The first conclusion drawn from the simulations of the initial phase of the pandemic was the need to consider the existence of a very significant asymptomatic population. Thus, in the classical model it is possible to obtain a rapid expansion of the pandemic simply by considering high values of the infection rate (β).
On the contrary, in the discrete model the application of existing data did not justify the observed data, unless there was a very significant asymptomatic population that hid the true magnitude of the spread of the infection. The symptomatic population in the early stages of the pandemic should be considered to be small. This, together with the data on spread through different geographical areas and the possible probability of infection, produced temporary results of much slower expansion that did not even trigger the priming of the model.
In summary, the result of the simulations led to totally inconsistent scenarios, until a high population of asymptomatic people was included, from which the model began to behave according to the observed data. At present, there are already more precise statistics that confirm this behavior that, in the group of infected people, get to establish that 80% are asymptomatic, 15% are symptomatic that require some type of medical attention by means of treatment or hospital admission and, the rest, 5% that require from basic level life support to advanced life support.
These figures help explain the virulence of a pandemic, which is strongly regulated by the percentage of asymptomatic individuals. This behavior justifies the enormous difference between the behaviors of different types of viruses. Thus, if a virus has a high morbidity it is easy to track and isolate, since the infectious cases do not remain hidden. On the contrary, a virus with low morbidity keeps hidden the individuals who are vectors of the disease, since they belong to the group of asymptomatic people. Unlike the viruses mentioned above, COVID-19 is a paradigmatic example of this scenario, with the added bonus that it is a virus that has demonstrated a great capacity for contagion.
This behavior has meant that when the pandemic has shown its face there was already a huge group of individual vectors. And this has probably been the origin of a chain of events with serious health, economic and social consequences.
The mechanisms of expansion and containment of the pandemic
In retrospect, the apparent low incidence in the first few weeks suggested that the risk of a pandemic was low and not very virulent. Obviously, an observation clearly distorted by the concealment of the problem caused by the asymptomatic nature of the majority of those infected.
This possibly also conditioned the response to their containment. The inadequate management of the threat by governments and institutions, the lack of protection resources and the message transmitted to the population ended up materializing the pandemic.
In this context, there is one aspect that calls for deep attention. A disease with a high infectious capacity requires a very effective means of transmission and since the first symptoms were of pulmonary type it should have been concluded that the airway was the main means of transmission. However, much emphasis was placed on direct physical contact and social distance. The minimization of the effect of aerosols, which are very active in closed spaces, as is now being recognized, is remarkable.
Another seemingly insignificant nuance related to the behavior of the pandemic under protective measures should also be noted. This is related to the modeling of the pandemic. The classical SIR model assumes that the infection rate (β) and recovery rate (γ) are uniquely proportional to the sizes of the populations in the different States. However, this is an approach that masks the underlying statistical process, and in the case of the recovery is also a conceptual flaw. This assumption determines the structure of the differential equations of the model, imposing a general solution of exponential type that is not necessarily the real one.
By the way, the exponential functions introduce a phase delay, which produces the effect that the recovery of an individual occurs in pieces, for example, first the head and then the legs!
But the reality is that the process of infection is a totally stochastic process that is a function of the probability of contagion determined by the capacity of the virus, the susceptibility of the individual, the interaction between infected and susceptible individuals, the geographical distribution, mobility, etc. In short, this process has a Gaussian nature.
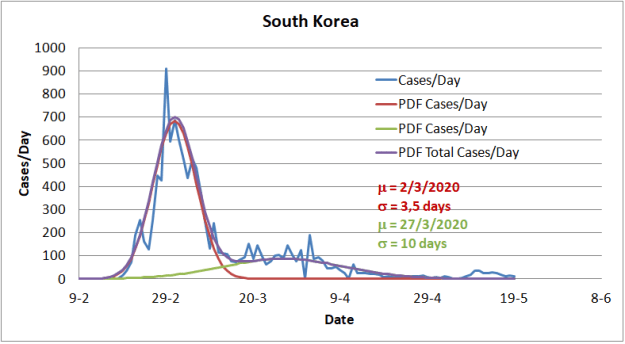
As will later be justified, this Gaussian process is masked by the overlap of infection in different geographical areas, so they are only visible in separate local outbreaks, as a result of effective containment. An example of this can be found in the case of South Korea, represented in the figure below.
In the case of recovery, the process corresponds to a stochastic delay line and therefore Gaussian, since it only depends on the temporary parameters of recovery imposed by the virus, the response of the individual and the healing treatments. Therefore, the recovery process is totally independent for each individual.
The result is that the general solution of the discrete SIR model is Gaussian and therefore responds to a quadratic exponential function, unlike the order one exponential functions of the classical SIR model. This makes the protection measures much more effective than those exposed by the conventional models. So they must be considered a fundamental element to determine the strategy for the containment of the pandemic.
The point is that once a pandemic is evident, containment and confinement measures must be put in place. It is at this point that COVID-19 poses a challenge of great complexity, as a result of the large proportion of asymptomatic individuals, who are the main contributors to the spread of infection.
A radical solution to the problem requires strict confinement of the entire population for a period no less than the latency period of the virus in an infected person. To be effective, this measure must be accompanied by protective measures in the family or close environment, as well as extensive screening campaigns. This strategy has shown its effectiveness in some Asian countries.
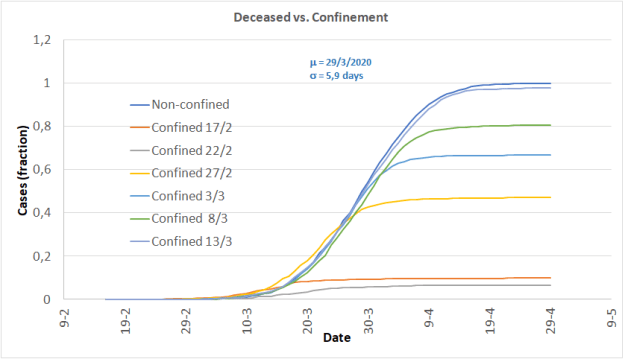
In reality, early prophylaxis and containment is the only measure to effectively contain the pandemic, as the model output for different dates of containment shows. Interestingly, the dispersion of the curves in the model’s priming areas is a consequence of the stochastic nature of the model.
But the late implementation of this measure, when the number of people infected in hiding was already very high, together with the lack of a culture of prophylaxis against pandemics in Western countries has meant that these measures have been ineffective and very damaging.
In this regard, it should be noted that the position of the governments has been lukewarm and in most cases totally erratic, which has contributed to the fact that the confinement measures have been followed very laxly by the population.
Here it is important to note that in the absence of effective action, governments have based their distraction strategy on the availability of a vaccine, which is clearly not a short-term solution.
As a consequence of the ineffectiveness of the measure, the period of confinement has been excessively prolonged, with restrictions being lifted once morbidity and mortality statistics were lowered. The result is that, since the virus is widespread in the population, new waves of infection have inevitably occurred.
This is another important aspect in interpreting the pandemic’s spread figures. According to the classic SIR model, everything seems to indicate that in the progression of the figures, a peak of infections should be expected, which should decrease exponentially. Throughout the first months, those responsible for the control of the pandemic have been looking for this peak, as well as the flattening of the integration curve of the total cases. Something expected but never seemed to come.
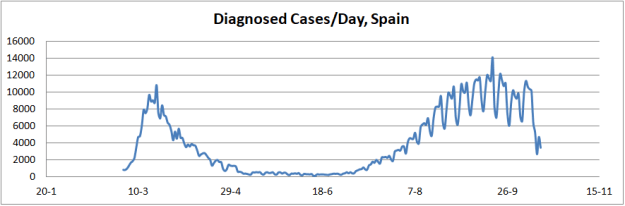
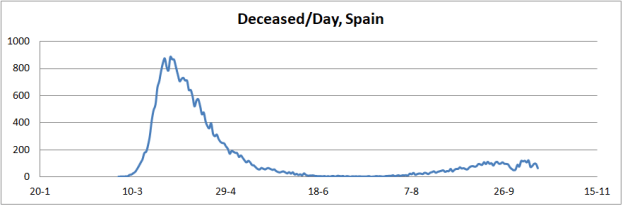
The explanation for this phenomenon is quite simple. The spread of the pandemic is not subject to infection of a closed group of individuals, as the classical SIR model assumes. Rather, the spread of the virus is a function of geographic areas with specific population density and the mobility of individuals between them. The result is that the curves that describe the pandemic are a complex superposition of the results of this whole conglomerate, as shown by the curve of deaths in Spain, on the dates indicated.

The result is that the process can be spread out over time, so that the dynamics of the curves are a complex overlap of outbreaks that evolve according to multiple factors, such as population density and mobility, protective measures, etc.
This indicates that the concepts of pandemic spread need to be thoroughly reviewed. This should not be surprising if we consider that throughout history there have been no reliable data that have allowed contrasting their behavior.
Evolution of morbidity and mortality
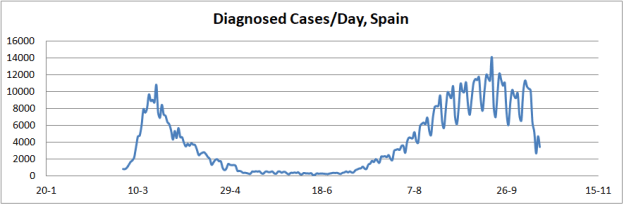
Another interesting aspect is the study of the evolution of morbidity and mortality of SARS-Cov-2. For this purpose, case records can be used, especially now that data from a second wave of infection are beginning to be available, as shown in the figure below.
In view of these data a premature conclusion could be drawn, assuring that the virus is affecting the population with greater virulence, increasing morbidity, but on the other hand it could also be said that mortality is decreasing dramatically.
But nothing could be further from reality if we consider the procedure for obtaining data on diagnosed cases. Thus, it can be seen that the magnitude of the curve of diagnosed cases in the second phase is greater than in the first phase, indicating greater morbidity. However, in the first phase the diagnosis was mainly of a symptomatic type, given the lack of resources for testing. On the contrary, in the second phase the diagnosis was made in a symptomatic way and by means of tests, PCR and serology.
This has only brought to light the magnitude of the group of asymptomatic infected, which were hidden in the first phase. Therefore, we cannot speak of a greater morbidity. On the contrary, if we look at the slope of evolution of the curve, it is smoother, indicating that the probability of infection is being much lower than that shown in the month of March. This is a clear indication that the protective measures are effective. And they would be even more so if the discipline were greater and the messages would converge on this measure, instead of creating confusion and uncertainty.
If the slopes of the case curves are compared, it is clear that the expansion of the pandemic in the first phase was very abrupt, as a result of the existence of a multitude of asymptomatic vectors and the absolute lack of prevention measures. In the second phase, the slope is gentler, attributable to the prevention measures. The comparison of these slopes is by a factor of approximately 4.
However, it is possible that without prevention measures the second phase could be much more aggressive. This is true considering that it is very possible that the number of vectors of infection at present is much higher than in the first phase, since the pandemic is much more widespread. Therefore the spread factor could have been much higher in the second phase, as a consequence of this parameter.
In terms of mortality, the ratio deceased/diagnosed seems to have dropped dramatically, which would lead to say that the lethality of the virus has dropped. Thus at the peak of the first phase its value was approximately 0.1, while in the second phase it has a value of approximately 0.01, that is, an order of magnitude lower.
But considering that in the figures of diagnosed in the first phase the asymptomatic were hidden, both ratios are not comparable. Obviously, the term corresponding to the asymptomatic would allow us to explain this apparent decrease, although we must also consider that the real mortality has decreased as a result of improved treatment protocols.
Consequently, it is not possible to draw consequences on the evolution of the lethality of the virus, but what is certain is that the magnitudes of mortality are decreasing for two reasons. One is virtual one, such as the availability of more reliable figures of infected people, and the other is real, as a result of improved treatment protocols.
Strategies for the future
At present, it seems clear that the spread of the virus is a consolidated fact, so the only possible strategy in the short and medium term is to limit its impact. In the long term, the availability of a vaccine could finally eradicate the disease, although the possibility of the disease becoming endemic or recurrent will also have to be considered.
For this reason, and considering the implications of the pandemic on human activity of all kinds, future plans must be based on a strategy of optimization, so as to minimize the impact on the general health of the population and on the economy. This is because increased poverty may have a greater impact than the pandemic itself.
Under this point of view and considering the aspects analyzed above, the strategy should be based on the following points:
- Strict protection and prophylaxis measures: masks, cleaning, ventilation, social distance in all areas.
- Protection of the segments of the population at risk.
- Maintain as much as possible the economic and daily activities.
- Social awareness: Voluntary declaration and isolation in case of infection. Compliance with regulations without the need for coercive measures.
- Implementing an organizational structure for mass testing, tracking and isolation of infected.
It is important to note that, as experience is demonstrating, aggressive containment measures are not adequate to prevent successive waves of infection and are generally highly ineffective, producing distrust and rejection, which is a brake on fighting the pandemic.
Another interesting aspect is that the implementation of the previous points does not correspond to strictly health-related projects, but rather to resource management and control projects. For this reason, the activities aimed at fighting the pandemic must be ad hoc projects, since the pandemic is an eventual event, to which specific efforts must be devoted.
Directing the effort through organizations such as the health system itself will only result in a destructuring of the organization and a dispersion of resources, a task for which it has not been created nor does it have the profile to do so.
